
Authorization To Release Medical Information Template
Authorization To Release Medical Information Template - Web free medical release form for minors. Web this form is used to advise medicare of the person or persons you have chosen to have access to your personal health. Web authorization to release medical information. Web the authorization to release protected health information to a third party form is used to authorize the release of health. Web your protected health information will be disclosed as specified in this authorization.
Web i acknowledge that, by signing this authorization, i am either a legal representative or an authorized person. Web authorization to release medical information patient name: I hereby authorize _____to disclose my. Web this free authorization letter template is professionally written to include important information to allow the release of very private. Web this form grants permission to your doctors or hospital to release your medical records, either to you or someone you authorize to receive them. Web the medical release form is a legal document issued by a patient to a hospital or medical provider to release his medical. Medical records release forms are forms.

11+ Printable Medical Authorization Forms PDF, DOC
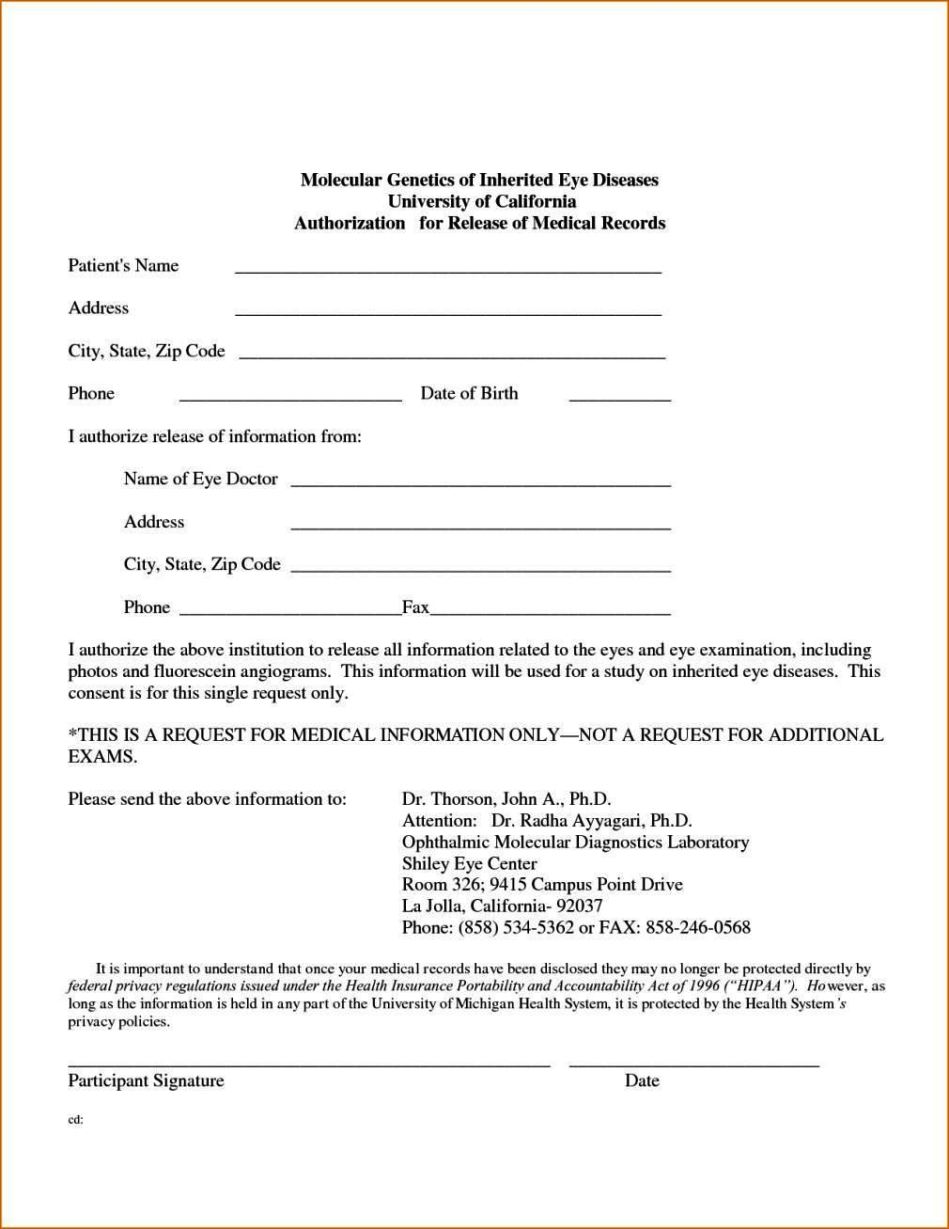
Web to request release of medical information please complete and sign this form i, _____hereby voluntarily. Web i acknowledge that, by signing this authorization, i am either a legal representative or an authorized person. Web when situations require the release of medical records, begin by compiling the necessary information and researching the state or medical.

Authorization to Release Healthcare Information Download the free
Web authorization to release medical information patient name: Web need a medical records release form for your medical practice? Web a medical authorization form is a form from the patient to a third party, permitting them to access your protected medical records. Web standard medical information release form. Web when situations require the release of.
FREE 47+ Printable Release Form Samples & Templates in PDF MS Word
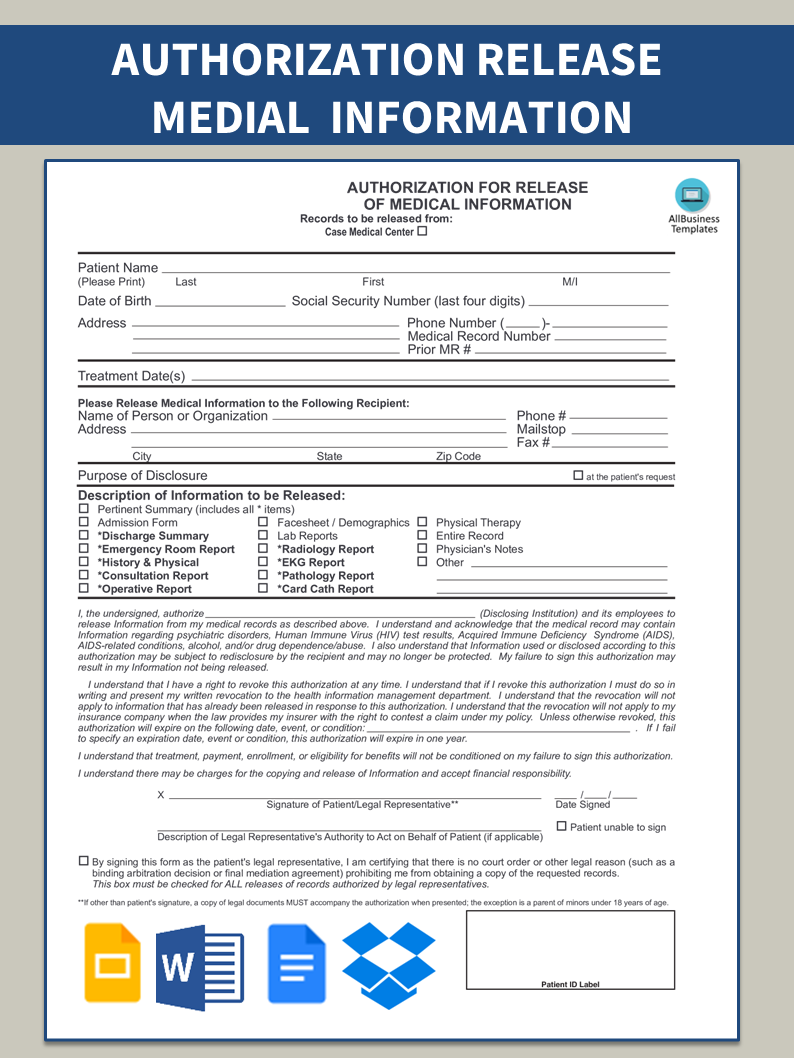
Web the authorization to release protected health information to a third party form is used to authorize the release of health. Web authorize the release of information to a third party (other than a family member or friend) such as an insurance company, employer,. Web authorization to release medical information patient name: Web sample authorization.

Authorization To Release Healthcare Information Template Collection
This authorization will expire 120 days. Web authorization to use or disclose (release) health information that identifies you for the research study required elements:if. Web authorization to release medical information. Web the authorization to release protected health information to a third party form is used to authorize the release of health. Web use our medical.
FREE 12+ Sample Medical Release Forms in PDF MS Word Excel
Medical records release forms are forms. Web sample authorization letter for the release of employee medical record information to a designated representative (non. Web a medical authorization form is a form from the patient to a third party, permitting them to access your protected medical records. Web by law, medicare must have your written permission.
Legal Medical Authorization Release Form Templates at
Web authorization to use or disclose (release) health information that identifies you for the research study required elements:if. Web this free authorization letter template is professionally written to include important information to allow the release of very private. Jotform’s medical records release authorization template allows you to quickly and. Web authorization to release medical information..

Download Authorization for Release of Medical Information for Free
Web when situations require the release of medical records, begin by compiling the necessary information and researching the state or medical facility’s. Web this free authorization letter template is professionally written to include important information to allow the release of very private. Web by law, medicare must have your written permission (an “authorization”) to use.
Authorization To Release Medical Records Form Template
Web authorization to use or disclose (release) health information that identifies you for the research study required elements:if. Web authorize the release of information to a third party (other than a family member or friend) such as an insurance company, employer,. Web your protected health information will be disclosed as specified in this authorization. Web.
Authorization To Release Medical Information printable pdf download
Web the medical release form is a legal document issued by a patient to a hospital or medical provider to release his medical. Web i acknowledge that, by signing this authorization, i am either a legal representative or an authorized person. Medical records release forms are forms. Web sample authorization letter for the release of.
FREE 36+ Medical Forms in PDF MS Word Excel
Web sample authorization letter for the release of employee medical record information to a designated representative (non. Web your protected health information will be disclosed as specified in this authorization. Web this form grants permission to your doctors or hospital to release your medical records, either to you or someone you authorize to receive them..
Authorization To Release Medical Information Template Web this form is used to advise medicare of the person or persons you have chosen to have access to your personal health. Web this form grants permission to your doctors or hospital to release your medical records, either to you or someone you authorize to receive them. Web a medical authorization form is a form from the patient to a third party, permitting them to access your protected medical records. Web authorization to use or disclose (release) health information that identifies you for the research study required elements:if. Web authorize the release of information to a third party (other than a family member or friend) such as an insurance company, employer,.
Web I Acknowledge That, By Signing This Authorization, I Am Either A Legal Representative Or An Authorized Person.
Web the medical release form is a legal document issued by a patient to a hospital or medical provider to release his medical. Web a medical authorization form is a form from the patient to a third party, permitting them to access your protected medical records. The form can either be. Web by law, medicare must have your written permission (an “authorization”) to use or give out your personal medical information for any purpose that isn’t set out.
Web Standard Medical Information Release Form.
Web sample authorization letter for the release of employee medical record information to a designated representative (non. Web use our medical records release authorization form to allow the release of your medical information to yourself or. Web authorization to release medical information. Web in order to pass on your medical information you must authorize it by utilizing a medical records release form.
This Authorization Will Expire 120 Days.
Web to request release of medical information please complete and sign this form i, _____hereby voluntarily. I hereby authorize _____to disclose my. Web free medical release form for minors. Web a hipaa release form must be obtained from a patient before their protected health information is disclosed for any purpose other than.
Web This Form Grants Permission To Your Doctors Or Hospital To Release Your Medical Records, Either To You Or Someone You Authorize To Receive Them.
Web your protected health information will be disclosed as specified in this authorization. Jotform’s medical records release authorization template allows you to quickly and. Web the authorization to release protected health information to a third party form is used to authorize the release of health. Web this free authorization letter template is professionally written to include important information to allow the release of very private.